

Previously unpublished data shows that people are not choosing MAiD simply because they are lonely.



Late last year, headlines claimed that hundreds of Canadians chose Medical Assistance in Dying (MAiD) simply because they were lonely1. It was a claim designed to shock—and it worked, sparking outrage and political talking points. We decided to see if it was true2. We spent months analysing BC government records, combing through over 30,000 individual data points3, and examining exactly what people report when they request MAiD4. The truth is nothing like the story that made the news.

The “lonely Canadian choosing to die” narrative is easy to sell. It’s a quick, shocking headline that fits neatly into a social media post or political soundbite. But it erases the complexity of MAiD and distorts public understanding of who chooses it and why. Behind every request is a person living with the realities of serious illness, irreversible decline, and suffering that cannot be eased in a way they find acceptable.
It’s true that loneliness and isolation are often part of that picture — just as they are for many older adults in Canada who do not choose MAiD5—but to present them as the driving force behind a request for MAiD is to miss the point entirely. These feelings are more often the shadow cast by other forms of suffering: losing the ability to move freely, care for oneself, engage in meaningful activities, or escape constant physical decline—and the data we obtained seems to make that clear.
Here’s our topline findings:
Track 1 - Reasonably foreseeable natural death
Of the 2,689 people who had MAiD under Track 1 in BC in 2023, 699 (26%) reported isolation or loneliness as one of their sources of suffering.
Of the 2,689 people in BC who had MAiD under Track 1 in 2023, only one reported isolation or loneliness as their sole source of suffering.
Track 2 - No reasonably foreseeable natural death
Of the 78 people who had MAiD under Track 2 in BC, 33 (42%) reported isolation or loneliness as one of their sources of suffering.
Of the 78 people in BC who had MAiD under Track 2 in 2023 , none reported isolation or loneliness as their sole source of suffering.
Just one person out of 2767 (0.036%) reported only isolation or loneliness, and they were in Track 1, not Track 2. In BC, not a single Track 2 case matched the news headlines.
However, the real story in the data turned out to be far more revealing than simply proving the headlines wrong. To see it, we first need to quickly revisit one of the core eligibility criteria—because that’s where the role of isolation and loneliness in a person’s suffering becomes clear.
MAiD Eligibility
To receive MAiD, a person must meet very specific legal requirements. While there are several criteria6, the one most relevant here is that they must have a “grievous and irremediable medical condition”—and, in particular, they must be experiencing intolerable suffering.
This means they must be experiencing enduring physical or psychological suffering that cannot be relieved under conditions they consider acceptable. That suffering has to be described in their own words and formally documented by MAiD assessors.
It’s this criterion —and how that suffering is reported—that sits at the heart of the media claims we’ve been examining.
Reported Nature of Suffering
The chart below breaks down the types of suffering reported in 20237, and it’s our starting point for understanding how loneliness and isolation actually fit into MAiD decisions. This data covers all of Canada, but as you’ll see below, these are comparable to data from BC only.
Before we look at the numbers, it’s worth remembering that this chart shows what people reported as part of their suffering —not necessarily the main reason(s) they chose MAiD.
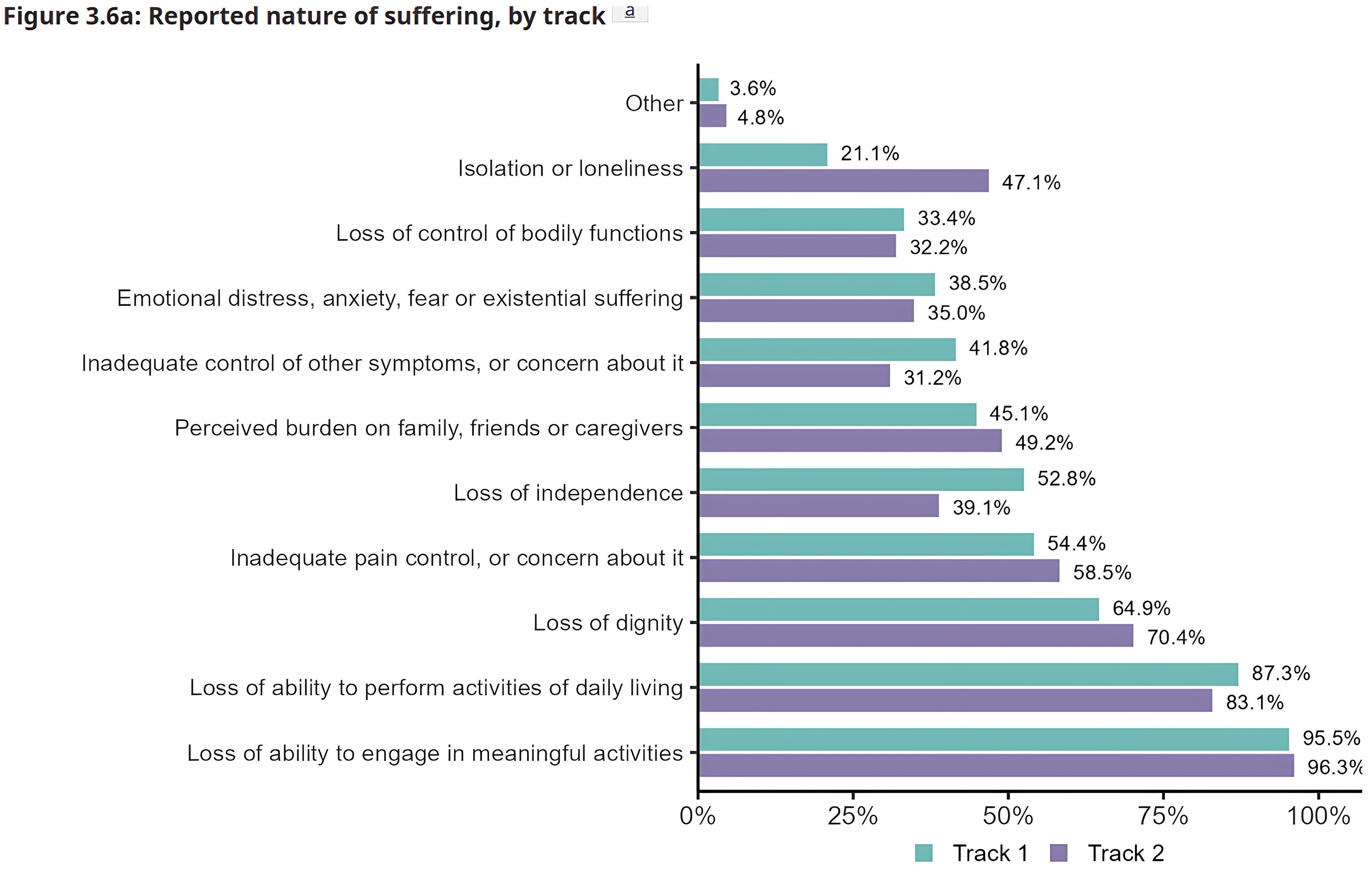
At first glance, the numbers seem to back up the headlines: 47.1% of people who had MAiD under Track 2 reported loneliness or isolation. That’s a striking figure—but it raises a critical question the chart can’t answer: was loneliness or isolation the reason they wanted MAiD?
It’s important to note that the percentages add up to more than 100%, because people can (and most often do) report multiple sources of suffering. That means we need to dig deeper. Specifically, we set out to answer three key questions:
How often is isolation or loneliness reported as the only type of suffering?
How is isolation or loneliness related to other types of suffering?
How does isolation or loneliness fit into the overall picture of a person’s suffering?
1. How often is it only isolation or loneliness?
We’ve already answered this. One out of 2767 cases in BC (and, if extrapolated to all of Canada, likely no more than six). Some might say that is still too many, and they might be right. But we know that the one in BC was a Track 1 case, so the person had to have an incurable medical condition with a reasonably foreseeable natural death.
We also know there is about a 60% chance that the incurable medical condition was cancer, a 20% chance it was cardiovascular disease, a 13% chance it was a neurological disease, a 13% chance it was respiratory failure…we think you get the point8. Are we really supposed to believe that someone living with advanced cancer or progressive neurological decline chose MAiD because they were lonely? Framing it that way isn’t just misleading—it’s a deliberate distortion of the reality these patients are facing. And the people pushing that narrative should know better.
2. How is isolation and loneliness related to other types of suffering?
The progression through the eligibility criteria is pretty easy to follow: as an example, a person might have Parkinson's (serious and incurable disease) which has lead to a significant dependence on aids for personal care and mobility (advanced state of irreversible decline) which has resulted in an inability to engage in meaningful activities or perform activities of daily living9 (the intolerable suffering)10.
If isolation or loneliness was reported in a case like this, we would argue it is actually a result of an advanced state of irreversible decline and intolerable suffering, rather than being the intolerable suffering itself: the intolerable suffering (inability to engage in meaningful activities or perform activities of daily living) has led to isolation and loneliness.
Is our argument supported by the data reported in the Fifth Annual Report on MAiD where news reports got their data? Unfortunately, no. Which is why we needed data on what each individual who had MAiD reported as the nature of their suffering.
Here’s how that data breaks down:
Track 1 cases:
There were 2689 people who had MAiD under Track 1 in BC in 2023.
Of those 2689:
699 (25%) reported isolation or loneliness as one of their sources of suffering.
Of the 699 who reported isolation or loneliness:
134 (19%) also reported inability to engage in meaningful activities.
11 (2%) also reported inability to perform activities of daily living.
547 (78%) also reported BOTH inability to engage in meaningful activities AND inability to perform activities of daily living.
7 (1%) did not also report inability to engage in meaningful activities AND/OR inability to perform activities of daily living (though six did report other sources of suffering).
Ninety-nine percent of Track 1 MAiD patients who reported isolation or loneliness also reported being unable to engage in meaningful activities and/or perform activities of daily living. 99%!!
Track 2 cases:
There were 78 people who had MAiD under Track 2 in BC in 2023.
Of those 78:
33 (42%) reported isolation or loneliness as one of their sources of suffering.
Of the 33 who reported isolation or loneliness:
9 (27.3%) also reported inability to engage in meaningful activities.
1 (3%) also reported inability to perform activities of daily living.
23 (69.7%) also reported BOTH inability to engage in meaningful activities AND inability to perform activities of daily living.
One-hundred percent of Track 2 patients who reported isolation or loneliness also reported being unable to engage in meaningful activities and/or perform activities of daily living. 100%!!
In both Track 1 and Track 2 cases, the message is undeniable: isolation and loneliness almost never appear alone. Almost every single person who reported them was also facing serious losses in function and quality of life—the kind of suffering that defines eligibility for MAiD. So when critics point to “loneliness” as the reason people chose MAiD, they’re ignoring everything else those people were actually living with.
3. How does isolation or loneliness fit into the overall picture of a person’s suffering?
Our analysis found that isolation or loneliness is strongly linked to two other forms of suffering: an inability to engage in meaningful activities and/or an inability to perform activities of daily living. In almost every case where isolation or loneliness was reported, at least one of these other factors was present—often both.
That makes it hard to argue that isolation or loneliness is independently driving MAiD requests. The data strongly suggests the opposite: these feelings are more often the result of severe functional loss, and not the sole cause of the MAiD request.
Understanding what is driving what, matters11. If loneliness is an independent driver, the solution might be as simple as increasing social contact. But when it’s the byproduct of being unable to feed yourself, get out of bed, or take part in daily life, then simply increasing social contact leaves the underlying causes of suffering—the inability to engage in meaningful activities and to perform activities of daily living—unresolved.
Isolation and loneliness in MAiD cases are almost always the result of severe illness and functional loss — not the cause of the request.
Isolation and loneliness as an indicator of greater suffering
Another way to view this data is to ask whether isolation and loneliness appear more often when there is a greater overall level of suffering. Not all suffering is equal, and some types are related—for example, loss of bodily function and loss of dignity are closely related—but looking at the total number of causes of suffering reported can still reveal important patterns.
Across all Track 2 cases, the average number of sources of suffering reported was 5.13. If our suspicion is correct—that isolation and loneliness are the result of higher overall suffering—we would expect that average to be higher among those who reported them. That’s exactly what we found:
Isolation or loneliness: 6.42 sources of suffering
No isolation or loneliness: 4.60 sources of suffering
Difference: +1.82
For comparison, here’s how other forms of suffering ranked:
Perceived burden: 6.26 sources of suffering
No perceived burden: 4.53 sources of suffering
Difference: +1.73
That fits our argument: perceived burden, like isolation and loneliness, is likely the result of other sources of suffering, such as being unable to wash or feed oneself.
When we ask healthcare professionals what they think people report most often as their reason for requesting MAiD, the first answer is almost always pain.
Inadequate control of pain: 5.42 sources of suffering
No pain reported: 5.26 sources of suffering
Difference: +0.16
That’s not a meaningful difference at all.
How about symptoms other than pain?
Inadequate control of other symptoms: 5.75 sources of suffering
No other symptoms reported: 5.05 sources of suffering
Difference: +0.70
A bigger gap, but still less than half the difference seen for isolation and loneliness, and perceived burden.
The pattern is clear: isolation and loneliness consistently appear alongside a higher overall level of suffering—and to a greater degree than other items of similar prevalence.
Isolation and loneliness in MAiD cases tend to appear alongside a higher overall level of suffering.
What does this tell us?
Every way we look at this data tells the same story: isolation and loneliness are not the primary drivers of MAiD requests. While they are often reported, they seem to emerge as consequences of deeper suffering caused by serious illness and profound loss of function. When someone can no longer engage in meaningful activities or care for themselves, isolation and loneliness often follow, but it is highly unlikely these feelings alone are what lead to a MAiD request.
That said, we should absolutely be concerned about isolation and loneliness. But to suggest that preventing MAiD requests is as simple as keeping someone company is not just naive—it’s insulting. MAiD is almost never about loneliness; it’s about the relentless toll of illness, irreversible decline, and suffering no treatment can ease. Loneliness may be present, but it’s not the cause. It’s the echo of a life already narrowed by disease. The data makes that clear—not that clarity ever stopped a sensational headline. After all, “Dying Canadians driven by complex, unbearable suffering” doesn’t get the same clicks as “They chose death because they were lonely.”
We already knew this wasn’t true. Anybody even remotely involved with Medical Assistance in Dying in Canada could have explained to these “journalists” why is wasn’t true. All they had to do was ask—which they didn’t seem to care to do.
It takes a lot of time to actually examine the data to see if it tells us anything. It is way easier to to read a short report, find the most extreme way to interpret the data, and write about it. There is a reason our response is coming many months after the original news article—understanding takes time and effort.
Note that having an “advanced state of irreversible decline” does not necessarily mean that is also causing intolerable suffering. For some, the act of being cared for by family is an expression of love and connection; for others it might be intolerable. The only person that can say what is intolerable is the person experiencing it.
There’s a simple solution to all this: ask people to rank the suffering they’re experiencing. But of course, that will never—and should never—happen. Forcing someone already in profound distress to quantify each aspect of their suffering just to satisfy a political argument is both unethical and inhumane.
Thank you for this badly needed corrective. Here’s a piece I wrote in the Toronto Star recently about MAiD and mental disorders. https://www.thestar.com/opinion/contributors/maid-one-womans-legal-challenge-to-get-the-care-she-hopes-for/article_1b5e4dc8-f48a-11ef-912d-6fe6453d2756.html
great stuff! peace and love!